| Prevalence of Disorders | Preadolescents | Adolescents |
|---|---|---|
| Major depressive disorder | 2% | 5% |
| Dysthymia | 2% | 8% |
| Bipolar disorder | 0.3% | 1% |
Important Definitions
Note: Hypomanic-like episodes that are clearly caused by somatic antidepressant treatment should not count toward a diagnosis of bipolar II disorder.
According to the Diagnostic and Statistical Manual for Primary Care (DSM-PC) Child and Adolescent Version (Wolraich, M. (Ed.) 1996) , the following are the definitions for Sadness and Bereavement variations and problems:
Transient depressive responses or mood to changes in stress are normal in otherwise healthy populations.
Sadness or irritability that begins to include some symptoms of Major Depressive Disorders in mild form.
However, the behaviors are not sufficiently intense to qualify for a depressive disorder. These symptoms should be more than transient and have a mild impact on the child's functioning. Bereavement that continues beyond 2 months may also be a problem.
Presence of a single Major Depressive Episode. The Major Depressive Episode is not better accounted for by Schizoaffective Disorder. and is not superimposed on Schizophrenia, Schizophreniform Disorder, Delusional Disorder, or Psychotic Disorder Not Otherwise Specified.
There has never been a Manic Episode, a Mixed Episode, or a Hypomanic Episode.[note]
Specify (for current or most recent episode):
Severity/Psychotic/Remission Specifiers
Chronic
With Catatonic Features
With Atypical Features
With Postpartum Onset
Specify (for current or most recent episodes):
Severity/Psychotic/Remission Specifiers
Chronic
With Catatonic Features
With Melancholic Features
With Atypical Features
With Postpartum Onset
Specify:
Longitudinal Course Specifiers (With and Without Interepisode Recovery)
Recording Procedures
Recording Procedures, Depressive Disorders
Specify if:
Early Onset: if onset is before age 21 years
Late Onset: if onset is age 21 years or older
Specify (for most recent 2 years of Dysthymic Disorder):
With Atypical Features
Specify if:
Acute: if the disturbance lasts less than 6 months
Chronic: if the disturbance lasts for 6 months or longer. By definition, symptoms cannot persist for more than 6 months after the termination of the stressor or its consequences. The Chronic specifier therefore applies when the duration of the disturbance is longer to a chronic stressor or to a stressor that has enduring consequences.
Recording Procedures - Adjustment Disorders
Parent text for preschool children., Acute
Parent text for preschool children., Chronic
The Depressive Disorder Not Otherwise Specified category includes disorders with depressive features that do not meet the criteria for Major Depressive Disorder, Dysthymic Disorder, Adjustment Disorder with Depressed Mood, or Adjustment Disorder with Mixed Anxiety and Depressed Mood. Sometimes depressive symptoms can be present as part of an Anxiety Disorder Not Otherwise Specified. Examples of Depressive Disorder Not Otherwise Specified include:
Sadness related to a major loss. Typically persists for less than 2 months after the loss. However, the presence of certain symptoms that are not characteristic of a "normal" grief reaction may be helpful in differentiating bereavement from a major depressive disorder. These include guilt about things other than actions taken or not taken by the survivor at the time of death, thoughts of death, and morbid preoccupation with worthlessness.
Specify if:
Mixed: if symptoms meet criteria for a Mixed Episode.
Specify (for current or most recent episode):
Severity/Psychotic/Remission Specifiers
With Catatonic Features
With Postpartum Onset
Specify:
Longitudinal Course Specifiers (With and Without Interepisode Recovery)
With Seasonal Pattern (applies only to the pattern of Major Depressive Episodes)
With Rapid Cycling
Specify (for current or most recent episode):
Severity/Psychotic/Remission Specifiers
With Catatonic Features
With Postpartum Onset
Specify:
Longitudinal Course Specifiers (With and Without Interepisode Recovery)
With Seasonal Pattern (applies only to the pattern of Major Depressive Episodes)
With Rapid Cycling
Specify (for current or most recent episode):
Severity/Psychotic/Remission Specifiers
With Catatonic Features
With Postpartum Onset
Specify:
Longitudinal Course Specifiers (With and Without Interepisode Recovery)
With Seasonal Pattern (applies only to the pattern of Major Depressive Episodes)
With Rapid Cycling
Specify (for current or most recent episode):
Severity/Psychotic/Remission Specifiers
Chronic
With Catatonic Features
With Melancholic Features
With Atypical Features
With Postpartum Onset
Specify:
Longitudinal Course Specifiers (With and Without Interepisode Recovery)
With Seasonal Pattern (applies only to the pattern of Major Depressive Episodes)
With Rapid Cycling
Specify:
Longitudinal Course Specifiers (With and Without Interepisode Recovery)
With Seasonal Pattern (applies only to the pattern of Major Depressive Episodes)
With Rapid Cycling
Specify current or most recent episode:
Hypomanic: if currently (or most recently) in a Hypomanic Episode.
Parent text for preschool children.
Parent text for school age children.
Depressed: if currently (or most recently) in a Major Depressive Episode.
Parent text for preschool children.
Parent text for school age children.
Specify (for current or most recent Major Depressive Episode only if it is the most recent type of mood episode):
Severity/Psychotic/Remission Specifiers
Note: Fifth-digit coded cannot be used here because the code for Bipolar II Disorder already uses the fifth digit.
Chronic
With Catatonic Features
With Melancholic Features
With Atypical Features
With Postpartum Onset
Specify:
Longitudinal Course Specifiers (With and Without Interepisode Recovery)
With Seasonal Pattern (applies only to the pattern of Major Depressive Episodes)
With Rapid Cycling
The Bipolar Disorder Not Otherwise Specified category includes disorders with bipolar features that do not meet the criteria for any specific Bipolar Disorder. Examples include:
(See also: Nonmedication Alternatives for Your Child pt)
(See also: Medication Tables in Child Psychopharmacology DTW)
(See: A Parent's Guide to Bereavement pt)
Weller, RA, Weller EB, Fristad MA, et al: Depression in recently bereaved children prepubertal chidren AmJ Psychiatry 2: 418: 1536-1540, 1991.
Worden JW: Children and Grief: When a Parent Dies. New York, Guilford. 1996
Adapted from GLAD-PC* (Guidelines for Adolescent Depression in Primary Care Rachel Zuckerbrot Ed with permission. Edits for CHADIS by Raymond Sturner and Amy Cheung)
Epidemiology
Identification
Communicate with teens and parents:
Assess for impairment in: school, home, and peer settings (Curry, J 2006) . Subjective distress should also be assessed.
Severity is judged by the numbers of the 9 MDD symptoms & reported impairment as noted below:
| DSM-IV Guidelines for Grading Severity Depression | |||
|---|---|---|---|
| Category | Mild | Moderate | Severe |
| Number (of 9 MDD) symptoms | 5-6* | * | "most" |
| Severity of symptoms | Mild | * | Severe |
| Degree of functional impairment** | Mild impairment or normal functioning but with "substantial and unusual" effort | * | "Clear-cut, observable disability" |
| According to the DSM-IV-TR, Moderate episodes of depression "have
a severity that is intermediate between mild and severe." *Except consider severe even with "mild" in symptoms if: risk factors: presenting with of a specific suicide plan or recent attempt; psychotic symptoms; family history of first degree relatives with bipolar disorder, or severe impairment in functioning (such as unable to leave home). **Impairment > number of symptoms so: Severe = >6 >/=mild depressive symptoms & severe impairment |
|||
Differential Diagnosis for Depressive Disorders
Comorbidity with Depressive Disorders (See: Clinical Guide Algorithm)
General approach - Groundwork in the practice
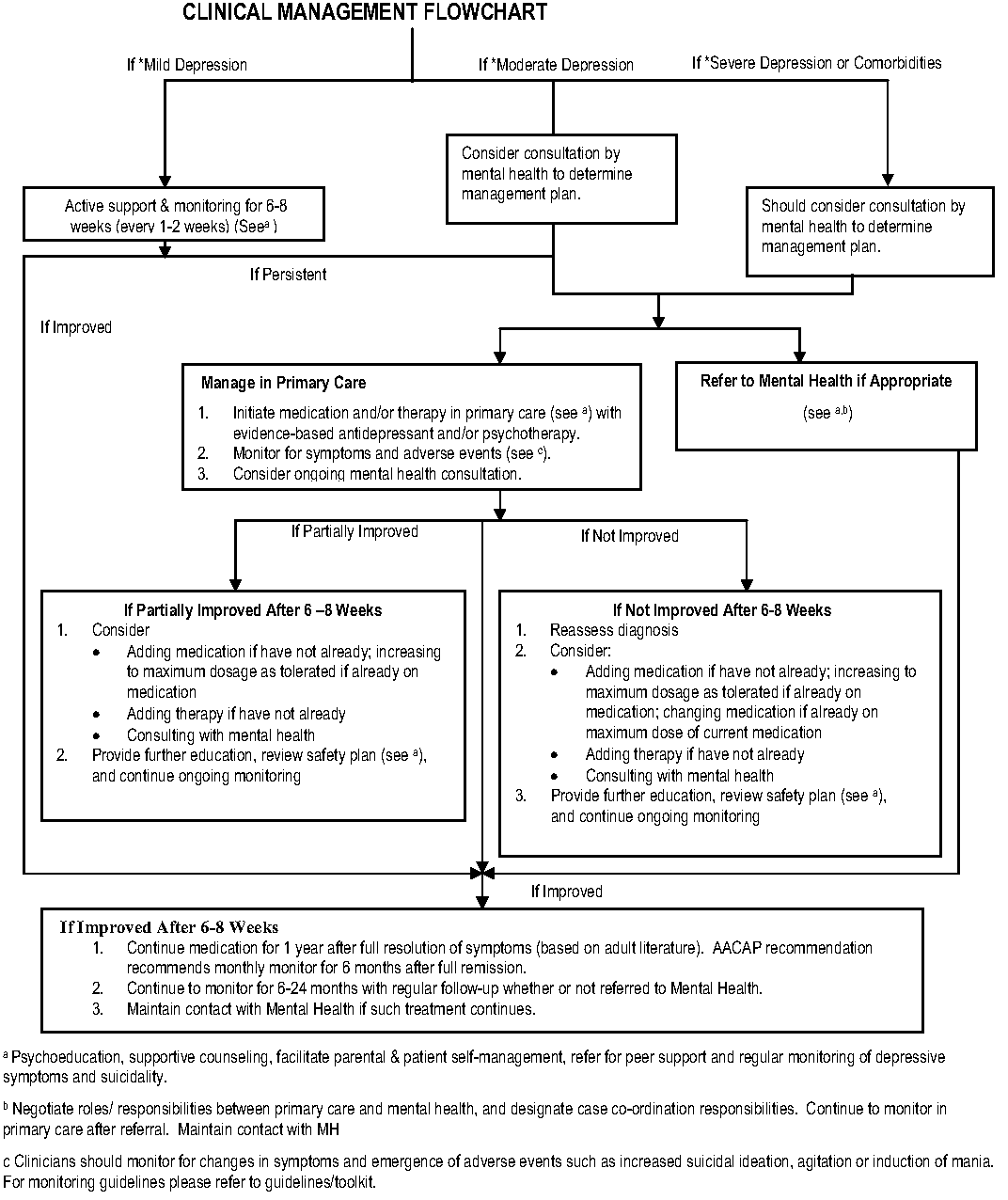
Treatment
First Priority = Safety Assessment and Planning
Educate and counsel families and patients about depression and options for the management of the disorder.
Treatment options for depression
Develop specific treatment plan
General Principles:
Treatment Options - based in part on severity assessment (See: Severity/Impairment Estimation)
New onset Mild
Mild Depression with moderate or severe or comorbidities such as substance abuse, recommend treatment, crisis intervention (as indicated), and mental health consultation immediately without a period of active monitoring.
Moderate depression with or without comorbid anxiety, consider consultation by mental health and/or treatment in the PC setting.
Severe: Referrals and Follow-up
Sequence in Referral Process
Treatment Choices: Supportive Counseling & Problem-Focused Therapy
Problem Solving Treatments for Primary Care (PST-PC)
Evidence-based Psychotherapy
Two "brands" of psychotherapy have been shown to be helpful for youth depression (see Table below):
Components of both CBT and IPT-A can usefully be included by experienced clinicians although they are designed to be given by highly-trained therapists as a "package".
| Therapy | Key Components | Manuals/Websites |
|---|---|---|
| CBT | -Thoughts influence behaviors and feelings, and vice versa.
Certain negative thoughts, such as pessimism and self-denigration,
evoke negative feelings that predispose to and/or are exacerbated in depression.
Treatment targets patient's thoughts and behaviors to improve his/her mood. -Essential elements of CBT include increasing pleasurable activities (behavioral activation), reducing negative thoughts (cognitive restructuring), and improving assertiveness and problem-solving skills to reduce feelings of hopelessness |
TREATING DEPRESSED CHILDREN: THERAPIST MANUAL FOR "TAKING ACTION"
Kevin Stark, Ph.D., and Philip C. Kendall, Ph.D., 1996 53pp., $13.00 ADOLESCENT COPING WITH DEPRESSION COURSE Gregory Clarke, Ph.D. Peter Lewinsohn, PhD Hyman Hops, Ph.D. ©1990 www.Kpchr.org |
| IPT | -Interpersonal problems may cause or exacerbate depression and that depression,
in turn, may exacerbate interpersonal problems. Treatment targets patient's
interpersonal problems to improve both interpersonal functioning and his/her mood. -Essential elements of interpersonal therapy include identifying an interpersonal problem area, improving interpersonal problem-solving skills, and modifying communication patterns. |
Interpersonal Psychotherapy for Depressed Adolescents, 2nd ed. Laura Mufson, Kristen Pollack Dorta, Donna Moreau, and Myrna M. Weissman. New York, Guilford Publications, 2004, 315 pp., $36.00. |
CBT=Cognitive Behavioral Therapy
IPT=Interpersonal Therapy
Evidence-based Pharmacotherapy
When to consider medication:
Before prescribing, assure:
Points to cover with parents and children are:
Medication Effectiveness Data
Selective Serotonin Reuptake Inhibitors (SSRIs)
Monitor for adverse events
Ongoing Management
Systematic and regular tracking of goals and outcomes from treatment
Follow-up visit should be within 1 week of start of meds.
Content at every visit should ask about:
Finding the optimal dose
Dosing is adequate when:
Increase dosage when:
Assess for side effects at each dose
Side effects of SSRI's:
Common
More serious side effects include the following:
| SSRI | Starting Dose* | Increments | Max Daily Dose | Contra-indicated Meds | Available Doses | RCT evidence for efficacy | Generic available |
|---|---|---|---|---|---|---|---|
| Fluoxetine (Prozac) | 10mg qd/od** | 10-20mg | 60mg | MAOIs | 10 mg tablets 10,20,40 mg pulvules 90mg weekly pulvule and liquid form |
Y*** | Y |
| Sertaline (Zoloft) | 25mg qd/od** | 12.5-25mg | 200mg | MAOIs | 25, 50, 100 mg tablets and liquid form | Y | N |
| Citalopram (Celexa) | 10mg qd/od** | 10mg | 60mg | MAOIs | 20, 40 mg tablets and liquid form | Y | Y |
| Escitalopram (Lexapro) | 5mg qd/od** | 5mg | 20mg | MAOIs | 5, 10, 20 mg tablets and liquid form | N | N |
| Fluvoxamine (Luvox) | 25 mg qd/od, ** then bid | 25 mg | 250mg | MAOI's, terfenadine, astemizole, pimozide | 25, 50, 100 mg tablets and liquid form | N | Y |
| * Start with lower doses for younger children; **qd = od = every day;
***Fluoxetine is FDA approved. FIRST LINE medications are Fluoxetine, Sertaline, and Citalopram. SECOND LINE medications are Escitalopram, and Fluvoxamine. |
|||||||
Changing Medication
| Medication | Tapering Increments | Time between each taper |
|---|---|---|
| Fluoxetine | 10 mg | 1-2 weeks |
| Sertraline | 25 mg | 1-2 weeks |
| Citalopram | 10 mg | 1-2 weeks |
| Escitalopram | 5 mg | 1-2 weeks |
| Fluvoxamine | 50 mg | 1-2 weeks |
| Paroxetine | 5 mg | 1-2 weeks |
*May start second medication but need to inform patients/families about possible adverse events such as serotonin syndrome
If no improvement after 6-8 weeks
If partial improvement
Maintaining Medication
In order to maintain medication the following is recommended:
Stopping Medication
When discontinuing medication, taper medication slowly. All SSRIs, with the exception of fluoxetine, should be slowly tapered when discontinued due to risk of withdrawal effects. See above table.
After stopping medication for depression
Suicidality in Adolescents and the Black Box Warning, (Adapted from the APA / AACAP's PhysiciansMedGuide)
Suicidality in Adolescents: Suicidal ideation and suicide attempts are common in adolescence and do not have the same prognostic significance for completed suicide as those behaviors in later life. Quoting data from the Youth Risk Behavior Study, the federal Centers for Disease Prevention and Control (CDC), reports that 17% of adolescents think about suicide in a given year. Among high school students, 12% of girls and 5% of boys attempt suicide in a given year. (Available at http://www.cdc.gov/HealthyYouth/YRBS/pdfs/trends-suicide.pdf. Accessed 12/29/2004) Ultimately, 2 per 100,000 girls and 12 per 100,000 boys die as a result of such attempts - a ratio of attempts to completed suicides is 6,000 to 1 among girls and 400 to 1 among boys. In the U.S., this translates into approximately 2000 young people who die each year as a result of suicide. Fortunately, however, the overall rate of suicide in the 10-19 year age range has declined by 25% over the past decade. Since this decade has been associated with a dramatic increase in the prescription rates of the newer SSRI antidepressants, a recent study has demonstrated that a 1% increase in prescription of antidepressant medication was associated with a 0.23 per 100,000 decrease in adolescent suicides. (Olfson M, Shaffer D, Marcus SC, Greenberg T. (2003). Relationship between antidepressant medication treatment and suicide in adolescents. Arch Gen Psychiatry 60:978-982.)
The Black Box Warning: In 2004, the FDA reviewed detailed reports of 23 clinical trials involving more than 4,400 children and adolescents who had been prescribed any of nine antidepressants for treatment of major depression, anxiety, or obsessive-compulsive disorder. (T.A. Hammad. Results of the Analysis of Suicidality in Pediatric Trials of Newer Antidepressants. Presentation at the FDA Center for Drug Evaluation and Research (CDER), Bethesda, MD. September 13, 2004. Available at: www.fda.gov/ohrms/dockets/ac/cder04.html#PsychopharmacologidDrugs. Accessed January 5, 2005.) No suicides occurred in any of these trials. The FDA concluded that more of the children and teens who were receiving an antidepressant medication spontaneously reported that they thought about suicide or made a suicide attempt than did those who received a placebo. At the same time, systematic measures of suicidality were available from 17 of the 23 studies. The FDA's analysis of these data found that medication did not increase suicidality that had been present at the start of the study, and that it did not induce new suicidality in those without prior suicidal ideation.In fact, all studies showed a reduction in suicidality over the course of treatment.
The FDA's analysis showed that about 2 out of 100 children not taking medication would spontaneously report suicidal thoughts and/or behaviors, compared to 4 out of 100 who were taking medication. These rates need to be understood in the context of findings from community samples cited previously in which as many as half or more of teenagers with major depression are thinking about suicide at the time of diagnosis and some 16% to 35% have made a previous suicide attempt. Although only nine medications were re-examined in the analysis, the FDA applied the labeling changes to all antidepressant medications. This was done on the basis of the advisory committee's concern that applying the warning only to the newer antidepressants reviewed would give doctors and patients the false impression that older antidepressants such as TCAs had a more favorable risk-benefit ratio.
The diagnostic codes for Major Depressive Disorder (Single Episode and Recurrent) are selected as follows:
In recording the name of a diagnosis, terms should be listed in the following order: Major Depressive Disorder, specifiers coded in the fourth digit (e.g., Recurrent), specifiers coded in the fifth digit (e.g., Mild, Severe with Psychotic Features, In Partial Remission, as many specifiers (without codes) as apply to the most recent episode (e.g., With Melancholic Features, With Postpartum Onset), and as many specifiers (without codes) as apply to the course of episodes (e.g., With full Interepisode Recovery); for example, 296.32 Major Depressive Disorder, Recurrent, Moderate, With Atypical Features, With Seasonal Pattern, With Full Interepisode Recovery.
Adjustment Disorders are coded according to the subtype that best characterizes the predominant symptoms:
Coding Note: In a multiaxial assessment, the nature of the stressor can be indicated by listing it on Axis IV (e.g., Divorce)
The diagnostic codes for Bipolar I Disorder are selected as follows:
In recording the name of the diagnosis, terms should be listed in the following order: Bipolar I Disorder, specifiers coded in the fourth digit (e.g., Mild, Severe with Psychotic Features, In Partial Remission), as many specifiers (without codes) as apply to the most recent episode (e.g., With Melancholic Features, With Postpartum Onset), and as many specifiers (without codes) as apply to the course of episodes (e.g., With rapid Cycling); for example, 296.54 Bipolar I Disorder, Most Recent Episode Depressed, Severe With Psychotic Features, With Melancholic Features, With Rapid Cycling.
Note that if the single episode of Bipolar I Disorder is a Mixed Episode, the diagnosis would be indicated as 296.0x Bipolar I Disorder, Single Manic Episode, Mixed.
To find the comment in-context, please follow the provided links.
{kind=link}
{kind=link}